AARP estimates that three out of four Americans over the age of 50 are planning…

Termination of Home-Health Care Services Is Becoming More Common
Many Americans are getting their Medicare benefits cut as home health providers, including occupational, speech, and physical therapists, social services, as well as skilled nurses are saying: “Your husband (or whomever) is not going to get better, so we will have to discontinue our services as Medicare will not pay for it.” Termination of care is swift, often within 48 hours of delivering the message, and the home health care chores fall to the family system or must be paid for out of family funds. So what changed?
Significant changes began on January 1, 2020, as to how Medicare pays for home health services. Medicare has altered its billing approach from a therapy delivered model (the more therapy you receive, the higher the payments billed to Medicare) and changed it into a reimbursement system known as the Patient-Driven Groupings Model, or PDGM. Medicare Advantage plans have separate rules and are not affected.
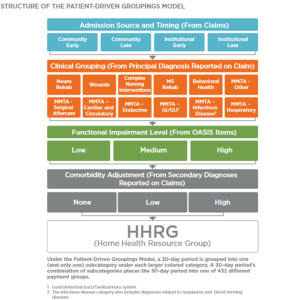
The Centers for Medicare and Medicaid Services (CMS) provide Figure 1 as an example of how a 30 day period becomes categorized into 432 case-mixed groups for adjusting payment purchases in the PDGM. These 30 day periods are further broken into the following subgroups: admission sources and timing, twelve clinical principal diagnosis subgroups, three functional impairment levels, and three levels of co-morbidity adjustments. During the 30 days, there is only an allowance for one chosen category under the larger color-coded categories. CMS deems this newer approach to be more holistic regarding patient need assessments.
In 2017, the most recent year for which the data is available, for-profit US home health care agencies (approximately 12,000) provided care to 3.4 million Medicare beneficiaries. Home health rates charged were based on the amount of therapy delivered. The more therapy a patient received, the higher the payout to the agency. Due to the change in payment structure, these agencies are cutting back on therapies provided and even reducing the number of therapists employed. They can’t bill enough to Medicare to remain profitable. These new payment conditions are based on a patient’s underlying diagnosis and other case-specific complicating medical factors. As a result, home health care agencies now have a stronger financial incentive to meet the needs of short-term therapy, post-hospital or rehab facility, as well as caring for patients requiring nursing care for complex situations like post-surgical wounds.
CMS believes this new way to assess payments will strike a balance between costs, efficiencies, needs, and outcomes. The members of the National Association for Home Care and Hospice (NAHC) disagree. Data culled by NAHC from home health agencies indicate there will be a substantial reduction of therapy services offered as a result of the PDGM. William Dombi, the association’s president, states that the cuts “may not be a good move” because medically, patients may deteriorate more rapidly without therapy and seek aid in emergency rooms or hospitals. He also notes the possibility that if more patients end up worse off and go to emergency rooms or hospitals, that this will reflect poorly on home health agencies and can affect their referrals.
Providing the right patient therapy at the right time by home health care agencies is critical to positive patient outcomes. CMS has done extensive analysis of historical data and, through the use of artificial intelligence tools, feel they can better predict what kind of services and how often a patient will need them through the PDGM. Clarifications are being posted online by CMS that deal with early errors in the program and the ensuing turmoil of therapy provision for patients within the new guidelines. It is the hope that more reviews and revisions to the PDGM will strike a better balance between cost and efficiency, patient therapy needs, and outcomes.
Understanding the role Medicare will play when it comes to long-term care services can be confusing. We help families plan for the possibility of needing long-term care, and how it could be paid for without causing the family to spend everything they have. If you’d like to discuss your particular situation, please don’t hesitate to reach out. Please contact our New York office or call us at 607-271-9270.
Related Posts


